Therapies that act synergistically are needed to significantly promote longevity

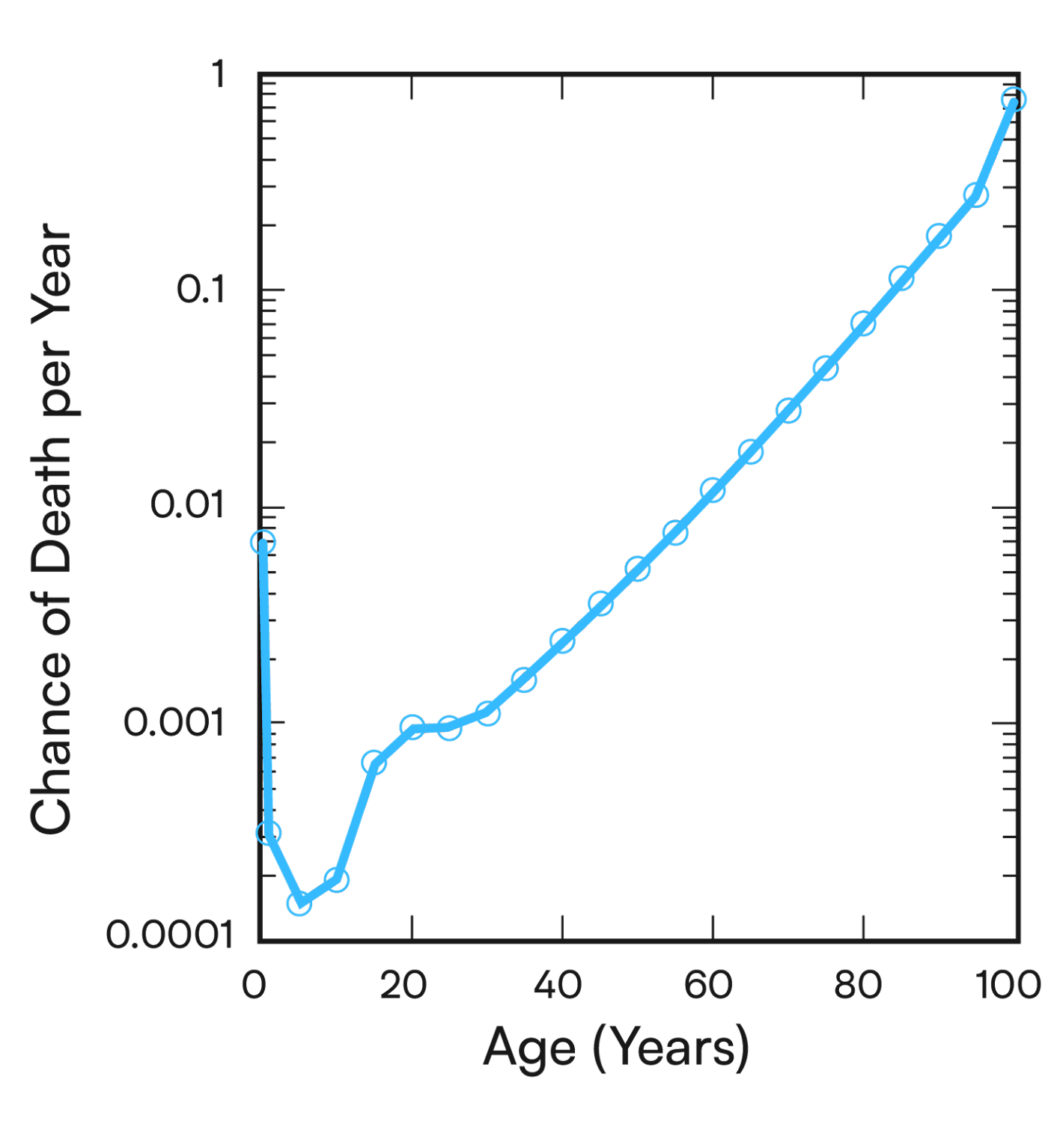
The math behind the expression “aging is inevitable” is the Gompertz-Makeham law. This law describes the probability of death as a function of age. It reaches 99.9+% by the time we are 100. One doesn’t need to know math to realize this, but because you’re here the underlying formula is an exponential function.
“Aging is a math problem — multiplicative therapies is the answer.”
Exponents involve multiplication. Another way this can be understood is that multiple factors synergize to make us die. Factors like smoking, drinking, poor sleep, bad diets have multiplicative effects. They don’t add together. Like an evil 401K, they compound to kill us. Aging is a math problem — multiplicative therapies is the answer.
“Understanding that it is factors that synergize to cause us to die will be key to fixing how we make therapies.”
Understanding that it is factors that synergize to cause us to die will be key to fixing how we make therapies. For many decades now, since the rise to prominence of rational drug design, there has been a fixation on identifying silver bullet therapies. That is, if we can just find the right target and then drug it strongly and selectively enough, we can cure disease. The invention of Gleevac, which targeted the gene mutation BCR-ABL for the cancer type CML, added fuel to this fire. (You too can cure disease if you can just make your drug as good — potent, selective — as Gleevac!).
From the joke above, you can tell the CML example created a false expectation. CML is a monogenic disease. Targeting the single mutant gene with a single agent worked there, but it has nothing to do with polygenic diseases that are most diseases we care about (Alzheimer’s, most other common cancers, heart disease, etc.). The case is similar with two of the blockbuster drugs of the past decades — statins and ACE inhibitors. Those drugs have one job — to move a number down (cholesterol or blood pressure, respectively). That is not what’s being asked of most other drugs.
“Rapamycin is a start, but it is unlikely to promote the transformative longevity gains we are aiming for.”
For longevity, the current best case drug is rapamycin. Rapamycin has a 10–20% effect on lifespan in animals. Do the exercise and review the literature for other small molecules for any disease model. You’ll see that 20% improvements are a best case scenario in general. 20% is not good enough, especially because animal experiments are done in highly controlled conditions that are optimized to find an effect if there is one to be detected. This won’t be the case in people. All this is to say — Rapamycin is a start, but it is unlikely to promote the transformative longevity gains we are aiming for.
The longevity community needs to learn from the cancer community. More recently, the cancer community is focusing on synthetic lethality. “Synthetic” is a terminology geneticists use to describe what I’m referring to as synergistic or multiplicative.
What is a multiplicative therapy? I mean agents that have profound effects on physiology when combined. Their effects are not additive. They are multiplicative. 20 X 20, not 20 + 20. The former is 10X the effect of the latter. The Yamanaka four factors are perhaps the first bona fide example of a multiplicative longevity therapy. Combining four genes that can convert any cell to an embryo! Fortunately, people are already starting to leverage this technology to turn back the clock of old cells. Other strategies involving combinations of small molecules are emerging too.
“The radical view through the Overton window is that the FDA should require that a therapy hits multiple targets in order to be approved.”
The recently approved ALS drug, which is the only disease modifying drug for this fatal condition, is a combination of two agents. It’s not even known molecularly how they work! Considering one of the most valuable drugs ever Aspirin has 23 putative targets, I’m not sure why we haven’t done more to normalize ‘irrational’ drug design. The radical view through the Overton window is that the FDA should require that a therapy hits multiple targets in order to be approved. Otherwise I think if one soberly surveys what gets approved these days the cost/benefit analysis won’t be good. Even the aforementioned ALS drug, despite how promising it might be, is not sustainably priced at $158,000 per year.
Statins and blood pressure meds are what I call ‘counting’ medications. All we care about is the number going down. We’re rarely doing addition. We need to stop counting and start doing multiplication. Just as cancer needs synthetic lethality, aging needs synthetic vitality.
“Just as cancer needs synthetic lethality, aging needs synthetic vitality.”
At VitaDAO we are looking for multiplicative therapies. Rejuvenome is too. Here’s a starting list of projects doing multiplicative therapies. We’d love for you to add to the list.